By: Dr. Azuka Ezeike, MBBS, FWACS (Obstetrics and Gynaecology), MSc (Public Health), Freelance Medical Writer. Medical review by The DLHA Team

A black pregnant lady holding her bulging abdomen in her hands with side image showing common (cephalic) baby position .
Click on image to enlarge.
As pregnancy progresses, the way the baby lies in the womb of the baby varies because of many factors. It is usual for the position to vary in the early months of pregnancy because of the smaller size of the baby to the size of the womb and the water(amniotic fluid) At less than 28 weeks of pregnancy, about 25% of babies are in breech presentation, this number reduces to 1 in 25 in labour. This is because, towards delivery, the baby takes the best possible position to enable a smooth labour process.
While the position may not matter in the early months of pregnancy, the outcome of your pregnancy may be affected if the abnormal baby position persists till delivery. Most babies occupy the normal head-down position in the last few weeks of pregnancy. Any position other than this is considered abnormal.
This article aims to educate African women on the different positions a baby can take during pregnancy, the dangers and effects of abnormal baby positions and how they are managed.
To get started, let us get to know some common terms that are used in describing baby positions during pregnancy.
During your antenatal visits, you may hear your doctors and nurses describe the position of the baby using different terms. [1] Here are some of the terms:
Presentation: This is the part of the baby that lies close to your birth canal (see figure 1).
The presentation can be:
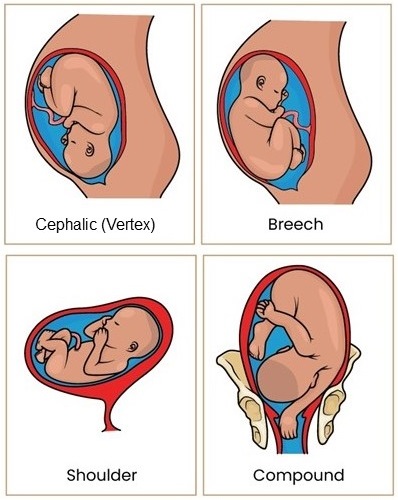
Figure 1: Showing types of foetal presentations during pregnancy. Click on image to enlarge.
Position: Refers to the direction of the baby’s skull in a cephalic presentation. There are three main positions (see figure 2):
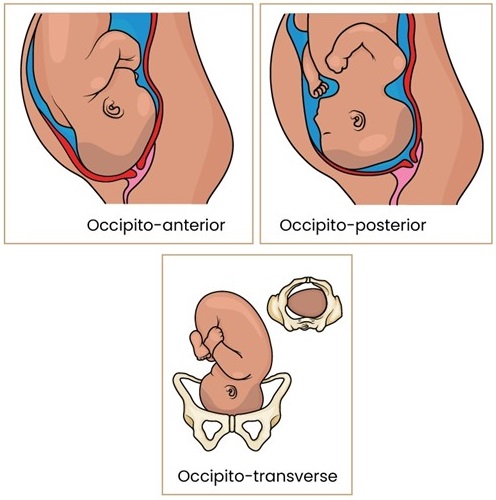
Figure 2 showing types of cephalic presentations. Click on image to enlarge.
Lie: This is how the baby is lying in the womb about the spine of the mother. There are three different types (see figure 3):
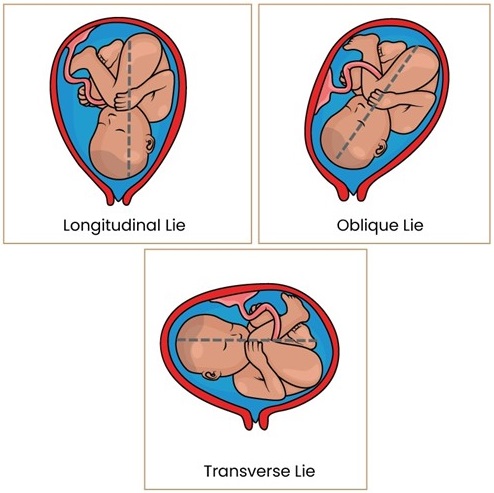
Figure 3 showing baby in different lie in the womb during pregmany. Click on image to enlarge
Most babies lie head down towards the end of the pregnancy. This is because of the pear-shaped nature of the womb. This gives more room in the upper part of the womb as the womb is more narrowed in the lower part. Because of this, the baby takes the position of best fit. The smaller head takes the narrow portion while the buttock which is broader and the limbs (legs) of the baby occupy the more spacious part of the womb. This is the cephalic presentation.
There are variants of the cephalic presentation, like:
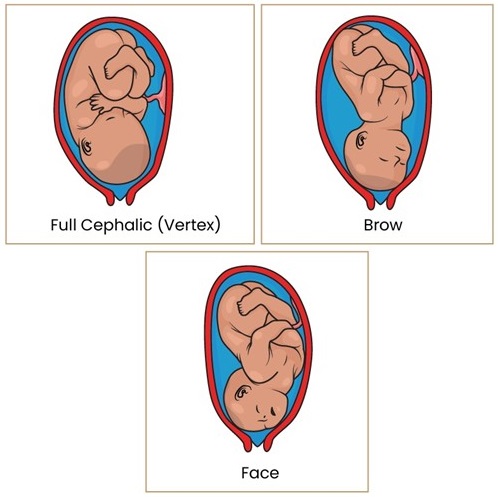
Figure 4: Showing variations in foetal cephalic presentation during pregnancy
Face presentation can be of two types:
Brow and face presentation can only be detected in advanced labour. [3]
Aside from the vertex (cephalic) presentation, every other baby’s position is considered abnormal. [4, 5]
These include:
Abnormal baby position if not well managed could lead to problems like:
Baby positions could be determined by your healthcare provider either during pregnancy or in labour.
During pregnancy, the way the baby is lying can be detected by your doctor or nurse through:
This involves the palpation (feeling or massaging) of the baby through your abdomen. Your healthcare provider feels the head as a firm, narrow, and somewhat mobile mass while the buttocks are felt as a broad, soft and fixed part of the baby. The limbs are felt as tiny, movable bumps inside the womb.
This uses soundwaves to detect the different parts of the baby and provides an image of their location in the womb on a computer screen.
However, some abnormal positions of the baby can only be detected with accuracy when you are in labour.
These include:
Some conditions may affect your baby’s position in the womb.
These are those that:
These conditions may be from the mother, the baby or from both mother and baby.
From the mother
From the baby
In some women, no definite cause can be found.
Abnormal baby position may be normal in early pregnancy as the baby is smaller and moves freely within the womb. As your pregnancy progresses and the baby gets bigger, the baby assumes a more stable position. This is usually around 36 weeks of pregnancy.
Therefore, if your baby is lying in an abnormal position before 36 weeks of pregnancy, there is no need for your doctor to do anything. Consider the case of Mrs. BN.
Mrs BN, is a 31-year-old woman in her third pregnancy who attended her antenatal care at a clinic at 33 weeks. Upon examination, she was informed that her baby was in a breech position. She returned home from the health facility in tears. On further review by a senior doctor, she was advised that there was no cause for alarm as the baby’s position would likely change before 36 weeks. At 36 weeks she was reexamined and it was confirmed that the baby had turned to head down position. She went on to have a normal vaginal delivery.
In a few women, this scenario may not be the reality as the abnormal position may persist till 36 weeks and beyond. If you find yourself in this condition, then there is a need for your healthcare provider to step in (intervene).
Your doctor would consider any of these options:
External Cephalic Version is a procedure that involves turning the baby from an abnormal position to the cephalic (head down) position.
The type of abnormal position that requires this procedure are:
The procedure would be done by your doctor under ultrasound guidance.
Before the procedure, your doctor would ensure that these conditions are met:
If these conditions are not met, the procedure may be difficult or dangerous.
If ECV fails or is not possible, your doctor will consider the other options.
Watch the video below to learn more about how ECV is performed
II. Vaginal Delivery
Vaginal delivery may be possible in these types of abnormal positions
In breech presentation, vaginal delivery may be considered if the following conditions are met:
Conducting breech delivery requires a lot of skills and success is only possible if the health worker taking the delivery is well skilled. Because of this, most doctors would prefer to deliver the baby through a caesarean section. Your doctor will advise you on the best option that you can choose.
Compound presentation, occipito-posterior position, brow presentation and face presentation may change to a normal presentation during labour and vaginal delivery will be possible.
However, if they persist or lead to prolonged labour, the option of caesarean section would be considered by your doctor.
III. Caesarean Section
This is considered if ECV and vaginal delivery are not possible. It is also considered if complications arise along the way. It involves the delivery of the baby by cutting through your abdomen and your womb. It is an operation that is considered safe in most instances, though problems may arise occasionally
Babies can take different positions in pregnancy depending on the age of the pregnancy and other factors. While normal positions demand no special actions (intervention) to be taken, an abnormal baby position requires some interventions to ensure that the pregnancy ends successfully. This is why you need to be enlightened so that you make informed decisions with the guidance of your health provider.
1. Okemo J, Gulavi E, et al, Abnormal lie/presentation. [Internet] 2021 February. In The Continuous Textbook of Women’s Medicine Series – Obstetrics Module, Vol 10. Glob. libr. women's med. DOI 10.3843/GLOWM.414593. Available from here.
2. Perkin RP. Compound presentations: Rare obstetric events. [Internet] 2024 May 24. [Cited 2024 Aug 20]; Available from here.
3. Makajeva J, Ashraf M. Delivery, face and brow presentation. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [Last updated 2023 Jan. 9]. Cited 2024 Aug 20. Available from here.
4. John Hopkins Medicine. Abnormal presentation [Internet, n.d.]. Cited 2024 Aug 20]. Available from here.
5. Pilliod RA, Caughey AB. Fetal Malpresentation and Malposition: Diagnosis and Management. Obstet Gynecol Clin North Am. 2017 Dec;44(4):631-643. doi: 10.1016/j.ogc.2017.08.003. Available from here.
Related: Essential Guide to Labour for African Women and Men
Published: October 15, 2024
© 2024. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution..
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


