Diabetes in Africa: Social Changes Fuelling Burden Rise
By: Arianna Russo, Freelance Health Writer and DLHA Volunteer. Editorially reviewed by the DLHA Team

Daily urban life scene in one of Africa’s megacities. Click on image to enlarge. Source
Urban Africa is undergoing a profound transformation. The rapid rise in type 2 diabetes across its cities is one of the clearest signs of this change, driven by social changes that extend beyond mere population density into the realm of daily life, culture, and health.
Traditional African lifestyles, long rooted in active routines and diets based on unprocessed foods, are increasingly giving way to modern habits influenced by rapid urbanisation and an extensive fast food consumer culture.
This change has created a complex health scenario.
While urbanisation brings undeniable benefits such as better infrastructure and job opportunities, it also fosters conditions conducive to chronic diseases. The growing prevalence of type 2 diabetes is an urgent warning of this ongoing public health crisis.
Beyond the rapid urbanisation, some of the other social factors shaping the rise in diabetes burden in African communities include (see fig. 1):
Many factors that include culture, belief systems. low investments in public health education, and low health knowledge among others contribute to the poor state of health literacy about diabetes care and prevention within African communities.
Health literacy is the ability to obtain, understand and use information and services in promoting self health and well-being.
Historically, African diets were dominated by fibre-rich grains, legumes, and vegetables. Physical activity was naturally integrated into daily life, like walking long distances, farming, or performing manual labor.
In contrast, today’s urban residents are more likely to consume high-calorie, ultra-processed foods and sugary drinks that are cheap and readily available in urban marketplaces and supermarkets.
.jpg)
Sugary drinks in plastic bottles are readily available and highly consumed by urban dwellers in many African cities.
At the same time, population growth, economic pressures, inequality and the growth of the service industry have led to more sedentary behaviours. Instead of walking to fetch water or working in the fields, many now sit for hours in offices and traffic, or at home, or street corners due to unemployment and underemployment. These lifestyle shifts and shocks, including the rise in alcohol consumption and smoking, are key contributors to obesity and insulin resistance, the two leading precursors of type 2 diabetes.
Africa’s healthcare systems have historically focused on combating infectious diseases like malaria, tuberculosis, and HIV/AIDS. The rapid rise in chronic conditions, particularly diabetes, presents a distinct challenge for systems that are under-resourced and inadequately equipped.
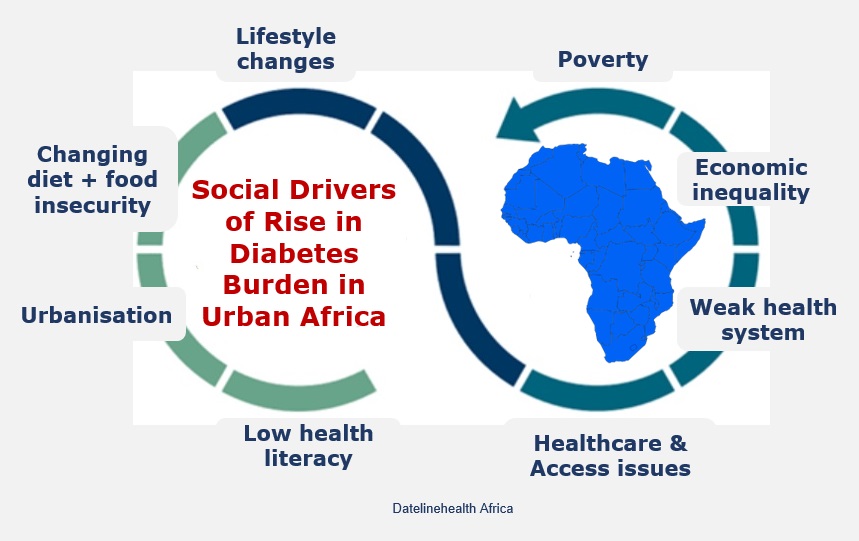
Fig. 1: Social drivers of rise in diabetes burden in urban Africa, Click on image to enlarge
Poorly resourced primary care clinics often lack the infrastructure, medications, and trained staff required to screen, diagnose, and manage chronic conditions. When coupled with other access challenges, late diagnoses and poorly managed disease progression becomes dominant. These in turn increase the risk of severe complications such as kidney failure, cardiovascular events, and limb amputations.
The long term cost of diabetes care imposes a heavy burden on both individuals and the economy. Out-of-pocket expenses for insulin, glucose monitors, and regular check-ups place an added and unequal financial strain on households which can push fragile families further into poverty. Poverty in turn promotes low education, chronic food insecurity, malnutrition, poor health and atypical diabetes. This feedback loop where poor health leads to educational, economic and nutritional hardship, in turn worsens health status and access to care.
Solving this crisis requires an integrated, diverse and practical approach involving governments, health systems, communities, and individuals. Below are key reform recommendations:
Governments should introduce fiscal and legal measures to influence food environments and support poverty reduction. These include:
Chronic disease screening and management must be integrated into routine care. Healthcare workers need training in diabetes prevention and patient-centered chronic care. Ensuring consistent and affordable medication and diagnostics supply chains, as well as affordable healthcare financing mechanisms are crucial.
City governments must prioritise urban design that promotes health. This includes:
Mobile health (mHealth) platforms can improve access to health information and support self-management for people with diabetes. SMS alerts, glucose monitoring apps, and remote consultations can extend the reach of health services to under-resourced communities.
The rise in the burden of diabetes in urban Africa is more than a medical concern, it is framed around socioeconomic factors with long-term implications for development. While urbanisation offers potential pathways to prosperity, without thoughtful interventions, it will continue to drive chronic disease profiles and inequality.
The future of Africa’s health lies in balancing modern progress with the wisdom of traditional lifestyles. Through informed policy, empowered communities, and reoriented health systems, the continent can turn the tide on diabetes epidemic and ensure that urban growth becomes a platform for well-being, not disease.
Mbanya JC, Motala AA, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375(9733):2254–66. Abstract available from here.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21. Abstract available from here.
Hu FB. Globalization of diabetes: the role of diet, lifestyle, and genes. Diabetes Care. 2011 Jun;34(6):1249–57. Available from here.
Steyn NP, McHiza ZJ. Obesity and the nutrition transition in sub-Saharan Africa. Ann N Y Acad Sci. 2014;1311:88–101. Available from here.
Bremner JD, Moazzami K, Wittbrodt MT, et al. Diet, stress and mental health. Nutrients. 2020;12(8):2428. Available from here.
Atun R, Davies JI, Gale EA, et al. Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 2017;5(8):622–67. Abstract available from here.
World Health Organization. Fiscal policies for diet and the prevention of noncommunicable diseases. Geneva: WHO; 2016.Available from here.
Related:
Published: August 26, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content freely for non-commercial purposes without alteration or modification and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


