By Chinedu Akpa. B. Pharm. Freelance Health Writer. Medicaly reviewed by: A. Odutola, MB.BS. PhD. FRCSEd.
.jpg)
Epilepsy in Africa. Click on the image to enlarge.
The nervous system which is made of billions of nerve cells otherwise known as neurons send and receive signals through their electrical activities. When these electrical activities become excessive the body may react in ways seen in people living with epilepsy.
According to the World Health Organization (WHO) an estimated 50 million people have epilepsy globally. [1] The institution defines epilepsy as a noncommunicable disease characterized by repeated unprovoked seizures (jerks), which are often brief involuntary movements that may affect a part of the body or the whole body. The seizures can cause loss of consciousness and loss of control of bowel and bladder functions. [2]
A lot of myths and misinformation abound in sub-Saharan Africa about the causes and treatments of epilepsy. These often delay access to improved healthcare services and hinder public health efforts at combating the scourge of this illness.
This article will provide you with the basic information you need to know about the types, symptoms, diagnosis, and treatment of epilepsy. At the end, it will provide you with links to reliable information about common myths and misconceptions and the facts you need to know to dispel them. In addition, it will also direct you to valuable first aid tips that you can use to support and protect someone having an epileptic seizure.
Epilepsy is a brain disorder that occurs when extensive and disorganised electrical signals (discharges) from cells of the brain occur spontaneously, without provocation and inhibition. [3] These electrical discharges occur in uncontrolled and uncoordinated ways that would explain the symptoms experienced during an epileptic attack.
The balance of electrical activity in the brain is regulated by two chemicals, called neurotransmitters. These are Glutamate and GABA (Gamma amino butyric acid).
Glutamate is a strong stimulant of nerve cell activity, while GABA strongly inhibits the same. Epilepsy arises when the brain releases too much glutamate with little or no inhibitory effects of GABA, making nerve cells of the brain discharge excessively.
Not everyone that has an uncontrolled and uncoordinated seizure or jerks is suffering from epilepsy as there are different types of seizures. So, how can you tell the difference between epilepsy and other seizures?
This question forms one of the basis of the myths and misconceptions about epilepsy, where it is assumed that everyone who suffers any form of seizure must be epileptic. To put this into perspective, about 30% of adults who are diagnosed with epilepsy are found to have non-epileptic seizures after proper assessment at an epilepsy center. [4]
Table 1 below summarizes the clinical differences between epileptic and non-epileptic seizures. [5, 6]
.jpg)
Table 1: Showing a comparison of the clinical features of epileptic and non-epileptic seizures. Click on the image to enlarge.
The reasons for the classification of epilepsy is to aid diagnosis and treatment. This is because some drugs are more effective in managing certain seizure types than others. Factors such as nature of onset, pattern of seizure, family history, brain electrical wave patterns or electroencephalogram (EEG), and magnetic resonance imaging (MRI) findings are considered during classification.
Clinicians generally use the International League Against Epilepsy (ILAE) classification system to diagnose and treat epileptic patients.
The most recent revision to the classification was completed in 2017. The updated edition categorizes epilepsy by four types as listed below.
For simplicity, it is the seizure type categorization that will be described in detail here as the classification of epilepsy usually starts first with the classification of the seizure type and then the epilepsy and syndrome type, followed by the cause of the epilepsy, where that is known. See fig. 1 for a flow pathway for the classification of epilepsy according to the ILAE.
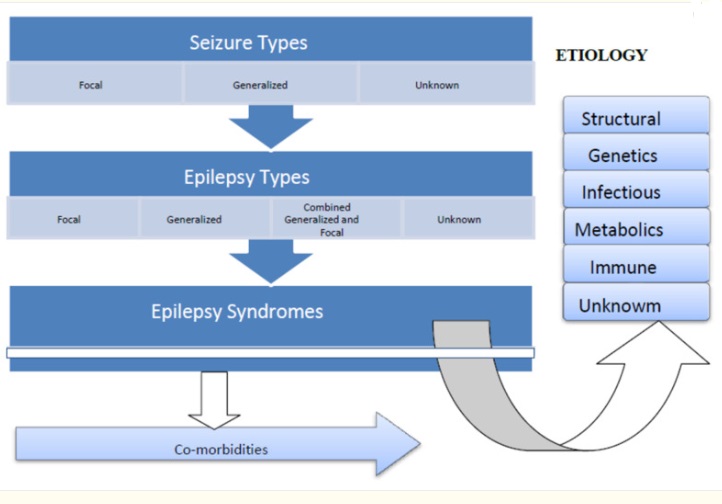
Figure 1: ILAE Classification of epilepsy 2017. Click on the iamge to enlarge. Credit.
Seizure type classification is based on the:
A seizure based classification can be divided into three categories as follows (see fig 2):
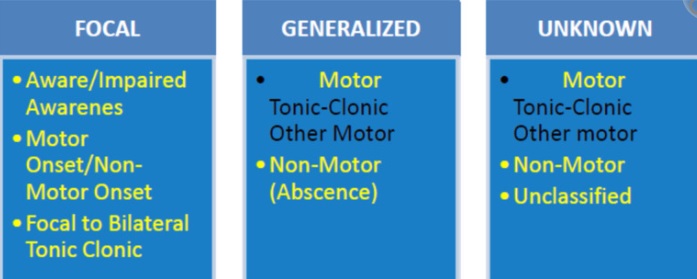
Figure 2: Basic classification of seizure type. Click on image to enlarge. Credit
This kind of seizure can have motor or non-motor appearance. It typically occurs when abnormal electrical activity starts in and is limited to a local area of one half of the brain. This may show up in the body as uncoordinated and uncontrollable muscle twitches or jerks in a particular region of the body or abnormal sensations in a specific part of the body or specific behaviour described in association with the seizure.
Focal seizures or epilepsy can happen in a patient who is aware (i.e., conscious) of their own symptoms or other happenings around them. Their memory for the event is intact. When this occurs, focal aware seizure (FAS) is the term used to describe this type of seizure. [7]
However, in other situations of focal seizures, the patient may not be aware (or conscious) of everything going on around them and memory for the event is lost. This is known as focal impaired awareness seizure (FIAS). [7]
Although a focal seizure is associated with localized signs (or observations), the effects may subsequently spread beyond a local area to involve the whole body. In which case the terms Focal seizure with generalization or Focal to bilateral tonic clonic seizure are used. [7]
In this type of seizure, abnormal electrical activities start spontaneously in a region of the brain and spread immediately to involve the entire brain, thereby causing generalised effects in the body. [7]
Generalised seizures can occur with or without muscle movements.
When it occurs without muscle movement (i.e. non-motor), it is known as typical or atypical Absence seizure.
Typical absence seizures are usually brief, with sudden loss of awareness (consciousness) wherein a patient stares blankly for a few seconds. This may be accompanied by minor muscle movements. [7] This is common in children and usually lasts for less than 10 seconds and may recur as much as few to multiple time in the day.
On the other hand atypical absence seizures last longer (usually more than 10 seconds) and may involve greater muscle movements like hand movement. A person affected by this type of seizure may respond more slowly to stimuli when compared to typical seizures and it tends to begin more slowly. [7]
When generalized seizures occur with muscle movements (i.e., motor), the following different types of movements may be observed:
Seizures that cannot be described by the patient because they occur during sleep are classified as Unknown. Those that are too difficult for the patient to explain are termed as Unclassified. When an ECG is done in these cases it might show normal results, which makes it difficult for a diagnosis to be made. More information will be needed for diagnosis for these types of seizures..
The classification of epilepsy types follow the general pattern described in classification of seizure types and include:
Epilepsy syndromes describe types of epilepsy with unique clinical features and brain waves that may have their onset at different stages of life from newborn and infancy through childhood and adulthood.
Further consideration of these types of epilepsy is beyond the scope of this article. Some general information is available here.
Signs and Symptoms of Epilepsy
For the lay public especially in Africa, one of the scary and embarrassing things about epilepsy is that the condition can occur anywhere without notice. If you're someone living with epilepsy, you will be advised against engaging in activities like driving and hiking.
The signs and symptoms can be very subtle (indistinct) and may vary depending on the seizure type. They include the following:
Certain conditions and engaging in certain activities can trigger your epilepsy symptoms. These triggers may include:
The diagnosis of epilepsy is not always easy as your doctor would need to gather several information in order to do so accurately.
A proper diagnosis requires that your doctor establishes your type of seizure and classify it accurately in order to provide treatment that is effective and right for you.
The benchmarks for accurate diagnosis of epilepsy include: [2]
In fulfilling these benchmarks, the first step in the diagnosis of epilepsy is for your doctor to obtain a thorough history and conduct a comprehensive physical examination on you.
Next, your provider may order additional tests in support of the clinical assessment. These tests may include such basic laboratory tests like Complete blood count, Blood chemistry tests, Spinal lumbar tap to collect cerebrospinal fluid (CSF) for study, Brain electrical activity test or Electroencephalography (EEG), Computed tomography (CT) imaging, Positron emission tomography (PET), and Magnetic resonance imaging (MRI), etc.
Even when the additional tests show nothing of interest, your healthcare provider can still make a diagnosis of epilepsy based on your symptoms only.
Epilepsy is not curable. So, the goal of treatment of epilepsy is to achieve seizure-free status without any negative consequences. This is typically accomplished in over 60% of patients. [8]
The approaches to treating epilepsy are three-pronged and include:
Medications used to manage epilepsy are commonly referred to as anticonvulsants or anti-seizure medications. They are usually prescribed when you have had more than one unprovoked seizure.
If you have had just one unprovoked seizure, and your EEG and MRI are normal, your risk of recurrence may be as low as 15%. In which case you would not be placed on medication, but will be monitored for any recurrence. [8]
If you have had only one unprovoked seizure (especially focal seizure), but both your EEG and MRI are abnormal, then your risk of recurrence of unprovoked seizure within 2 years after your first unprovoked seizures would likely be in the higher range within 15-70?. In this case, your doctor may consider placing you on medication with monitoring. [8]
Typical, if you are under monitoring following just one unprovoked seizure, you would need to avoid such epilepsy triggers like alcohol and sleep deprivation [8]
Because of adverse side effects of anticonvulsant (anti-seizure) medications, you will typically be started on a single therapy (monotherapy) if you fit the benchmark for placement on medications. Identifying the type of seizure that you’re experiencing is important at this stage because a medication may work well for one kind of seizure but make another worse. As a result, anticonvulsant medications are now categorized according to the kinds of seizures they treat.
Ethosuximide is used if you only have Absence seizures. But if it presents with other seizure types like generalized tonic-clonic seizure, myoclonic seizures, the choices of drugs are Valproic acid, and Lamotrigine.
Carbamazepine, and Gabapentin are avoided in this seizure type because they may worsen the seizure. [8]
These types of seizures are usually managed with anticonvulsant agents with a wide range of activities. The drugs of choice are Valproic acid, and Topiramate,
Additionally, another treatment option for these seizure types is Vagus Nerve Stimulation. This involves the periodic stimulation of your Vagus nerve, a cranial nerve of the brain, following the implantation of a tiny electrodes wired to an electrical stimulating device placed near the front of the chest. When operational, the device helps individuals with epilepsy lessen their abnormal electrical brain activity. [8]
Other drugs including Cannabidiol, can also be added to the main listed drugs in managing these seizures.
In children with myoclonic seizures (Juvenile myoclonic seizures), topiramate, and valproic acid are the most appropriate with levetiracetam as a supplemental drug.
Drugs like phenytoin and carbamazepine, which are used to treat partial seizures, are not only ineffective in treating juvenile myoclonic seizures, but they may even make the condition worse. [8]
Drugs with wide range activities are typically used in these types of seizures. When compared to other medications, valproic acid is preferred because it is more effective than lamotrigine and is better tolerated by patients. However, severe birth defects and impaired cognitive development have been observed in pregnant women; therefore, before administering such a drug to a pregnant woman, the doctor must perform a risk-benefit analysis. [8]
There are many drugs of choice for this type of seizure. These drugs are used singly (mono therapy) and they include carbamazepine, lamotrigine, and others (first line drugs). Additions such as levetiracetam, and pregabalin, may be considered if the first line drugs fail to work. [8]
These approaches are usually employed when conventional anticonvulsant drugs have failed to achieve the desired seizure freedom or as complementary therapy to medications.
Managing drug resistant epilepsy is a big challenge in sub-Saharan Africa, due to several resource limitations. The ILAE has defined drug resistant epilepsy as the failure to achieve sustained seizure freedom despite the use of two anti-epileptic drugs either as single agents or in combination.
Although a detailed discussing on how to manage drug resistant epilepsy is beyond the scope of the article, it is important to state that a multi-professional approach involving physicians, surgeons, psychiatrists, neuropsychologists, pharmacists, dietitians, and specialist nurses is often needed.
Available management options for drug resistant epilepsy include a mix of medical and non-medical options as listed:
Epilepsy remains a major public health challenge in Africa, with the continent experiencing one of the highest prevalence rates globally. Several factors contribute to this concerning trend, creating significant gaps in epilepsy treatment. Below, we explore the key challenges:
The high cost of antiepileptic drugs (AEDs) and limited access to newer medications hinder effective epilepsy management. Many Africans struggle to afford these essential medications due to widespread economic hardship. Additionally, the inadequate supply chain for AEDs leads to frequent shortages, further compounding the problem.
A significant number of primary health care workers lack the necessary training to diagnose and treat epilepsy effectively. Misdiagnosis is common, with seizures often mistaken for other conditions or attributed to supernatural causes. This lack of expertise delays treatment and exacerbates patient outcomes.
In rural areas, accessing healthcare facilities equipped to handle epilepsy is challenging. Poor road networks, dysfunctional transportation systems, and the concentration of specialized services in urban centers make it difficult for rural populations to receive timely care. Furthermore, diagnostic tools such as electroencephalograms (EEGs) are scarce and often overused, leading to frequent equipment breakdowns.
Cultural beliefs and stigma surrounding epilepsy significantly impact treatment-seeking behavior. Many people associate epilepsy with spiritual forces, leading them to prioritize traditional or spiritual healers over medical interventions. This misinformation prevents effective management and contributes to societal isolation for those with the condition.
Africa faces a severe shortage of neurologists and other specialist professionals needed for the care of epilepsy patients. This gap has created opportunities for untrained individuals, including spiritual healers and traditional practitioners, to fill the void, often providing ineffective or harmful interventions.
Epilepsy is a neurological disorder causing recurrent seizures due to abnormal brain activity. It affects about 25 million people in Africa, where myths and misconceptions hinder proper treatment. Diagnosis involves tests like EEGs and MRIs, and treatment focuses on seizure control through medication, surgery, or non-medical options like vagal nerve stimulation. Raising awareness and improving education are crucial for better epilepsy management in Africa.
1. World Health Organization. Epilepsy. [Internet]. February 7, 2024. Cited October 22nd, 2024. Available from here
2. Kassahun Bekele B, Nebieridze A, Moses Daniel I, Byiringiro C, Nazir A, Algawork Kibru E, Wojtara M, Uwishema O. Epilepsy in Africa: a multifaceted perspective on diagnosis, treatment, and community support. Ann Med Surg (Lond). 2023 Nov 20;86(1):624-627. doi: 10.1097/MS9.0000000000001536. Available from here
3. Anwar H, Khan QU, Nadeem N, Pervaiz I, Ali M, Cheema FF. Epileptic seizures. Discoveries (Craiova). 2020 Jun 12;8(2):e110. doi: 10.15190/d.2020.7. Available from here
4. Epilepsy Society. Non-epileptic Seizures and functional (dissociative) seizures. [Internet} Updated August 2023. Cited. October 23rd, 2024. Available from here
5. Kiriakopoulos E. Understanding Seizures. [Internet]. Epilepsy Foundation. October 1, 2019. Cited October 24th, 2024. Available from here
6. John Hopkins Medicine. Medical Management of Epilepsy. [Internet, n.d.]. Cited October 25th, 2024. Available from here
7. Sarmast ST, Abdullahi AM, Jahan N. Current Classification of Seizures and Epilepsies: Scope, Limitations and Recommendations for Future Action. Cureus. 2020 Sep 20;12(9):e10549. doi: 10.7759/cureus.10549. Available from here
8. Medscape. Epilepsy and Seizure Treatment and Management. [Internet]. July 26, 2022. Cited October 25th, 2024. Available from here
Related:
Epilepsy: An Awareness Guide for Africans
Published: December 1, 2024
© 2024. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


