Facial shingles: What Africans need to know
By Chinedu Akpa. B. Pharm. Freelance Health Writer. Medically reviewed by: A. Odutola, MB.BS. PhD. FRCSEd.

Close-up of the face of a black individual showing a distinct line of discoloration on one side of the forehead and face, likely due to herpes zoster infection (facial shingles) .
Facial shingles or herpes zoster ophthalmicus (HZO) isn't a stand-alone disease; it is a disease that manifests as a result of shingles. The face area is the second most common location for shingles attack, after the torso or trunk. [1]
Herpes zoster ophthalmicus affects the ophthalmic or eye branch of a nerve of the brain, called the trigeminal or 5th cranial nerve. [2] Due to the possibility of long-term consequences like vision loss, your healthcare provider may treat HZO as a medical emergency.
Herpes zoster virus infection usually reactivates when the body's immune system is low or compromised for various reasons. It presents with the typical shingles, blisters, scabs and pain on one side of the face (typically the forehead, eyelid and nose).
The risk factors, management, and prevention of facial shingles are comparable to those described in detail here.
Facial shingles (HZO) do not occur in all people who get shingles. Similar to shingles elsewhere in the body, there is little information available on how common the condition is in Africa. However, approximately 4–20% of people with shingles worldwide are predicted to develop facial shingles at some point. Of this group, 1 in 4 (25%) are predicted to have a chronic or recurrent illness, and roughly 1 in 2 (50%) will likely develop an eye condition. [2]
Women are more likely than men to have shingles (HZ) and facial shingles (HZO] specifically. [2] Additionally, research has indicated that black people are marginally less likely to get shingles and consequently facial shingles. According to one study, older black people are nearly eight times less likely than their white counterparts to have shingles. Similar trends have also been consistently observed in children. [3]
When reactivated from its inactive or dormant state, the herpes zoster virus typically travels along a nerve pathway. Due to the nerve pathway it follows, the virus infection presents itself in a unique way on one side of the face, not crossing the midline. It may potentially affect two close dermatomes on one side. [4] As a result, one side of your face develops shingles blisters while the other side stays unaffected. It may also only affect the forehead and eyelid but it is more likely to affect your eyes if blister formation appears close to the tip of your nose (Hutchinson's sign). [4]
The typical symptoms of facial shingles or herpes ophthalmicus include:
Additional symptoms and signs of facial shingles include:
If you notice any of these changes, you should see your healthcare provider or an eye doctor promptly.
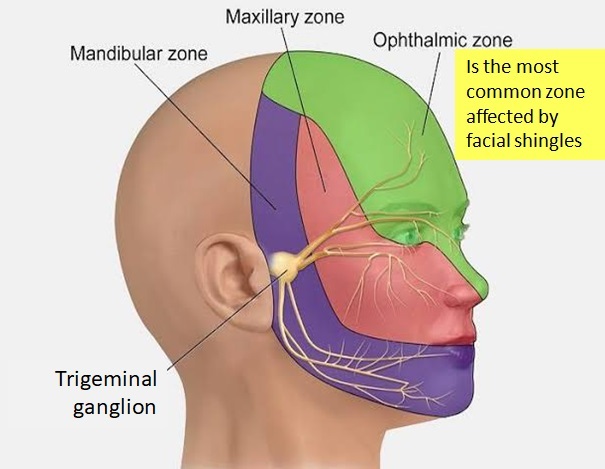
Diagram showing the distribution of the trigeminal nerve and its branches in the face. Click on image to enlarge.
The trigeminal nerve is the main sensory nerve of the head and face. It is located within the skull. It transmits information about touch, pain, temperature, and proprioception (muscle and joint positions sense) from the head and face to the brain. The nerve usually splits into three branches, each exiting the skull to various parts of the face, namely:
The ophthalmic and maxillary zones carry only sensory information while the mandibular carries both sensory and motor information like chewing.
When reactivated from its dormant (inactive) state, the virus can travel along any of the nerve branches but more often it affects the ophthalmic division that supplies the forehead, upper eyelid and nose areas of the skin of the face. It is unclear why this is so. [3]
Although the virus typically affects one side of the face (unilateral infection), it can also affect both sides (bilateral infection). This is however extremely uncommon, particularly in healthy individuals. [5]
The complications of facial shingles may include: [6]
HZO can be prevented with the Varivax or Shingrix vaccines. While Varivax is more suitable for children and immunocompetent adults, Shingrix is more suited for adults 50 years and above and those who are immune compromised.
Herpes zoster infection outbreaks typically go away on their own without any help. This happens more in children.
Oral antiviral agents may reduce the severity and the length of time of the symptoms. The following oral antiviral agents can be used to achieve this:
Other medications used to manage the associated pain, itching, and inflammation include:
Herpes zoster ophthalmicus (HZO) or facial shingles, is a subtype of shingles that commonly affects the ophthalmic branch of the trigeminal nerve ( a cranial nerve in the brain). This nerve carries sensations from the skin of the forehead, eyelids and nose sensations into the brain.
HZO causes typical facial pain and blisters of herpes zoster on one side of the forehead that may extend to the eyelid and nose.
Complications of HZO may include increased risk of stroke, damage to the cornea, and other tissues of the eye.
Treatment and prevention of HZO are similar to those provided by your healthcare provider for shingles generally.
1. Nair PA, Patel BC. Herpes Zoster. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from here.
2. Litt, J., Cunningham, A.L., Arnalich-Montiel, F. et al. Herpes Zoster Ophthalmicus: Presentation, Complications, Treatment, and Prevention. Infect Dis Ther 2024;13, 1439–1459. Doi: 10.1007/s40121-024-00990-7. Available from here.
3. Janninger, CA. Herpes Zoster. Treatment and Management. [Internet]. Medscape. Updated July 21,2021. Available from here.
4.Tuft S. How to manage herpes zoster ophthalmicus. Community Eye Health. 2020;33(108):71-72. Available from here.
5.Ng JM, Hsiao CH. Bilateral herpes zoster ophthalmicus in an immunocompetent patient. Eur J Ophthalmol. 2024 Jan;34(1):NP32-NP34. doi: 10.1177/11206721231177895. Available from here.
6. Lewis K, Palileo B, Pophal C, Yasmeh J, Glendrange R. Herpes zoster ophthalmicus. In Ophthalmic pearls. American Academy of Ophthalmology. [Internet]. Jan 1st, 2020. [Cited January 9, 2025]. Available from here.
Related:
Published: January 15, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


