By: Dr. Rahat Aisha Yasmeen, Freelance Health Writer and Datelinehealth Africa (DLHA) volunteer. Medical review and editorial staff provided by the DLHA Team.
Noma is a gangrenous (i.e., body tissue destroying), non-infectious and neglected disease that is also known by the following medical terms as Necrotizing ulcerative stomatitis, Gangrenous stomatitis, or Cancrum oris.
It is mainly widespread in sub-Saharan Africa, but sporadic cases are also reported in other parts of the world.
Initially, Noma begins with a soft tissue injury in the gums and inside the mouth (see figure 1).

Figure 1 showing early stage of Noma with soft tissue damage (ulcer) of the inside of the lower lip in an HIV-seropositive young male.
Click on image to enlarge. Credit.
The initial damage of the gums then develops into rapidly progressive destruction of the soft tissues (necrotizing ulcerative gingivitis) and progressing further to involve the surrounding hard tissues and skin of the face.
In 1994, WHO declared Noma as a public health problem with African children aged between 0 - 6 years being the most afflicted. In 1998, the WHO estimated that there were 140,000 new cases of Noma per year. According to a survey conducted in Africa in 2007 by WHO, 39 of the 46 Member States surveyed had cases of Noma reported over the past decades.
In Africa, especially south of the Sahara, there is a high prevalence of acute Noma or Acute Necrotizing Ulcerative Gingivitis (ANUG) in children that ranges from 15% to 60%, depending on the region and the degree of poverty.
Burkina Faso, Ethiopia, Mali, Niger, Nigeria and Senegal are the most disease affected countries – forming the “Noma belt” of the world. In these countries, an estimated annual occurrence rate is about 20 cases per 100,000.
Without treatment, Noma is fatal in 70 to 90% of cases due to dehydration and malnutrition.
The causative agent of Noma remains unknown.
It seems unlikely that a single infectious agent (virus or bacteria) is responsible for the disease.
Recent studies using special study (genomic) approaches showed an imbalance in the normal mouth microbes (organisms) with an overall loss of diversity.
More precisely, acute Noma seems to be characterized by a decrease in certain microbes in the mouth referred as Capnocytophaga and Fusobacteria genera and by the increase of Prevotella genus.
Noma is the result of complex interactions and associated risk factors.
According to the WHO, some of the multiple risk factors for Noma are listed in Table 1 below:
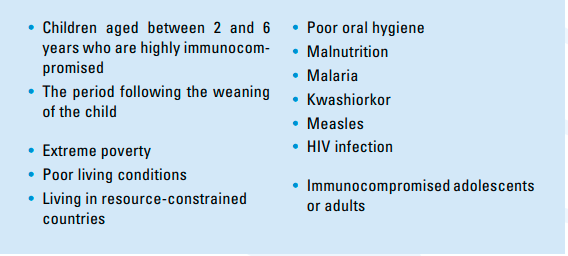
Table 1: Risk factors associated with Noma. Click on image to enlarge.
Depending on the stage of Noma, signs and symptoms vary as follows (see figure 2):
• Red or purplish red gum.
• Swelling and ulceration of the gums, and
• Foul breath or halitosis.
• Swelling or oedema inside (intra oral) and around (perioral) the mouth areas.
• Painful cheek.
• High fever.
• Excessive salivation.
• Mouth soreness.
• Difficulty during eating.
• Anorexia, and
• Pain and swelling of lymph nodes (Lymphadenopathy).
• Rapid perforation of the cheek.
• Presence of necrotic area with slough formation.
• Exposition of the teeth and denuded bones.
• Progressive drying of the facial gangrene.
• Anorexia.
• Apathy.
• Trismus (Lockjaw).
• Sequestration or loosening of teeth from the gums and exposure of bones and beginning of scarring tissue
• Difficulty eating.
• Speech problems.
• Salivary leakage.
• Teeth displacement.
• Dental anarchy (disfigurement).
• Fusion of the bones of the face (maxilla and mandible) and
• Nasal regurgitation (Food and saliva coming out of the nose).
.png)
Figure 2: Showing the stages of Noma. Click on image to enlarge.
When Noma is detected at an early stage, its progression can be stopped quickly with basic hygiene, antibiotics and nutritional rehabilitation. Such early detection helps prevent suffering, disability and death.
However, the vast majority of affected communities in Africa are located in peri-urban and rural areas where traditional beliefs and stigma prevail, and where early detection, diagnosis and access to care are difficult.
Survivors suffer severe facial disfigurements, have difficulty in speaking and eating, face social stigma and require complex surgery and rehabilitation.
• Mouthwash with chlorhexidine or betadine.
• Prescribe antibiotics such as amoxicillin and metronidazole.
• Use painkillers such as Paracetamol and Aspirin.
• Clean wound with saline or hydrogen peroxide and pack the inflamed areas with a compress.
• Use supplements such as Vitamin A, B and C and high protein intake.
• Encourage nutritional rehabilitation plus fluid and electrolyte correction to see quicker results as Noma patients are often dehydrated.
• Debridement (Removal and cleaning) of necrotic tissue and scabs
• Extraction of loose teeth and
• Rehabilitation and reconstruction of damaged face.
The simple answer is, yes; Noma can be prevented through the following ways:
• Public awareness and health literacy promotion regarding Noma prevention and control programs
• Active involvement of information in school curricula
• Educational and entertainment activities or initiatives at municipal or local facilities, including recreational facilities to promote primary prevention of Noma.
• Provision of access to daily essentials like water, sanitation and hygiene plays a key role in improving health of the society as whole.
• Nutritional support programs targeting children aged 0 - 6 years.
• Active engagement of community leaders to promote behavior change towards oral health will help prevention and early detection of Noma.
Other supporting prevention efforts include:
• Reducing the negative impact caused by the disease, such as social stigma, disability or death, through treatment and rehabilitation.
United Nations Human Rights Council Resolution 19/7 adopted on March 22, 2012 “The right to food,” advocated for the inclusion of Noma on the list of neglected tropical diseases to encourage more medical and institutional attention for this often lethal or very mutilating infectious gangrene.
Noma is an extreme and neglected disease affecting the most vulnerable children, especially in the tropics, with long term debilitating effects. This disease and its debilitating impacts are preventable with early detection and basic care. Noma should added to the WHO list of Neglected Tropical Diseases (NTD), to maximize its global monitoring and research
1. Evaluation of the WHO Africa Regional Programme on Noma Control (2013 - 2017). Accessed May 5 2023.
2. World Health Organization. Regional Office for Africa. A step-step guide to develop national action plans for Noma prevention and control in priority countries. WHO Regional Office. Brazzaville, 2020. Accessed May 5, 2023.
3. World Health Organization. Regional Office for Africa. Oral and dental health. WHO Regional Office. Brazzaville, 2014. Accessed May 5, 2023.
4. World Health Organization. Regional Office for Africa. Promoting Oral Health in Africa: Prevention and control of oral diseases and Noma as part of essential noncommunicable disease interventions. WHO Regional Office. Brazzaville, 2016. Accessed May 5, 2023.
5. Srour ML, Marck K, Baratti-Mayer D. Noma: Overview of a Neglected Disease and Human Rights Violation. Am J Trop Med Hyg. 2017 Feb 8;96(2):268-274. doi: 10.4269/ajtmh.16-0718. Epub 2017 Jan 16. PMID: 28093536; PMCID: PMC5303022.
6. Idigbe EO, Enwonwu CO, Falkler WA, Ibrahim MM, Onwujekwe D, Afolabi BM, Savage KO, Meeks VI. Living conditions of children at risk for Noma: Nigerian experience. Oral Dis. 1999; 5:156–162. [Abstract],
7. Baratti-Mayer D, Gayet-Ageron A, Hugonnet S, François P, Pittet-Cuenod B, Huyghe A, Bornand JE, Gervaix A, Montandon D, Schrenzel J, Mombelli A, Pittet D, Geneva Study Group on Noma (GESNOMA). Risk factors for Noma disease: a 6-year, prospective, matched case-control study in Niger. Lancet Glob Health. 2013;1:e87–e96.
8. Bolivar I, Whiteson K, Stadelmann B, Baratti-Mayer D, Gizard Y, Mombelli A, Pittet D, Schrenzel J, Geneva Study Group on Noma (GESNOMA). Bacterial diversity in oral samples of children in Niger with acute Noma, acute necrotizing gingivitis, and healthy controls. PLoS Negl Trop Dis. 2012; 6:e1556.
9. Huyghe A, Francois P, Mombelli A, Tangomo M, Girard M, Baratti-Mayer D, Bolivar I, Pittet D, Schrenzel J, Geneva Study Group on Noma. Microarray analysis of microbiota of gingival lesions in Noma patients. PLoS Negl Trop Dis. 2013;7:e2453.
10. Khammissa, R.A.G., Lemmer, J. & Feller, L. Noma staging: a review. Trop Med Health 50, 40(2022).
Published: May 8, 2023
© 2023. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content without alteration or modification and subject to attribution as to source.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


