Type 2 Diabetes Mellitus in African Children
By: Chinonso Cynthia Ukah. BNSc, RN, RM, RPHN. Freelance Health Writer. Medically reviewed by A. Odutola, MBBS, PhD, FRCSEd.

A black father with his girl child on his lap. Image credit: Freepik
Type 2 diabetes mellitus (T2DM) used to be a disease seen primarily in adults and referred to as "adult-onset diabetes". But with its increasing prevalence in children, the term has become obsolete. [1]
The world is experiencing a rise in the number of children with type 2 diabetes. Many researchers attribute this phenomenon to the increasing obesity cases seen in children. [2]
Both adults and children with T2DM have similar risk factors and present with the same symptoms. However, the modes of treatment differ and children quickly present with complications more rapidly than adults. [2]
This article will explain what childhood type 2 diabetes mellitus is, its risk factors, signs and symptoms and the recommended ways of managing the disease.
Type 2 diabetes mellitus is a metabolic disorder that affects how the body processes glucose and responds to insulin. One in three children diagnosed with diabetes has type 2 diabetes mellitus (T2DM). [2]
Normally, when a child eats food that contains carbohydrates, certain cells (beta cells) of an organ in the abdomen, called the pancreas, release sufficient amounts of insulin to help move glucose (the end product of digestion) into the body's cells. This in turn produces energy for the child's growth, development, and daily activities.
In a child with type 2 diabetes, this normal process is altered. The beta cells still produce sufficient amounts of insulin but the body's cells are unable to respond to the effect of insulin. This is called insulin resistance.
Research has shown that insulin resistance may be present for some time before a child is diagnosed with type 2 diabetes mellitus. [2]
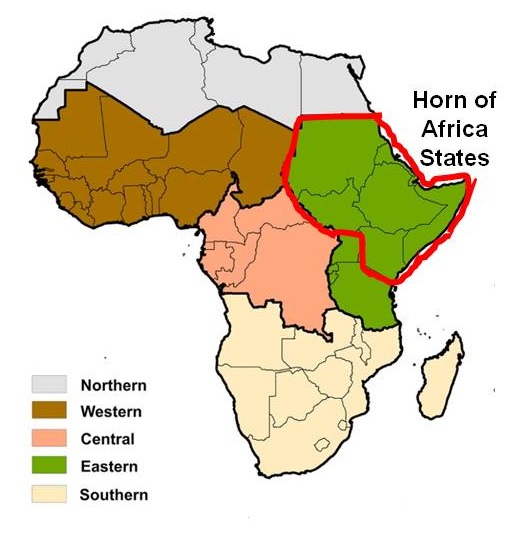
The Horn States of Eritrea and Sudan have the highest burden of Diabetes Mellitus in sub-Saharan Africa. Click on image to enlarge.
The burden of T2DM is increasing in African children, posing challenges to their growth and development. The highest burden is seen in States within the Horn of Africa (e.g., Eritrea, 11.2/100,000 population and Sudan, 10.3/100,000) , while the lowest is seen in West African (e.g., Nigeria, 3.1% and Cote d' Ivoire, 0.4%).
Despite a slight decline in the mortality rates of T2DM observed in West Africa, children continue to die from the disease and its complications.
These complications, which can present as kidney failure, cardiovascular diseases, or infections, are worsened by poor access to healthcare, late diagnosis, and limited awareness seen in many regions of Africa.
Research has shown that children with type 2 diabetes (T2DM) lose a significant number of healthy years (measured as Disability-Adjusted Life Years; DALYs) due to the impact of the disease. This includes years lost due to premature death as well as those affected by disabilities such as nerve damage, vision impairment, and amputations.
Specifically, Tanzania has the highest rates of childhood diabetes-associated DALYs.
Without proper intervention, the rising burden of childhood T2DM in Africa can have long-term consequences. It may increase healthcare costs and reduce the life expectancy of these children. [2] As of 2017, the life expectancy of children with diabetes in sub-Saharan (SSA) is an average of 5 years.
Therefore, it is important to recognize the signs and symptoms of the disease, as this will aid early and proper intervention.
Children with type 2 diabetes do not often know they have it. They hardly present with any indicators (symptoms) of the disease. However, you may observe the following conditions in the early phases:
Several factors expose African children to Type 2 Diabetes Mellitus. They include:
Obesity
Obesity is one of the major risk factors of type 2 diabetes in children. It is characterized by excessive accumulation of body fat, also known as adipose tissues.

An African mother holding and showing off her overweight baby. Image credit.
Obesity causes insulin resistance in many organs and tissues. This condition often leads to hyperglycaemia (increased glucose levels in the blood) and speeds up the progressive dysfunction and damage of pancreatic beta cells with time. [2]
The World Health Organization (WHO) in 2022 confirmed 160 million cases of obesity in children aged 5-19 years. Although childhood obesity appears to have stabilised, cases of childhood type 2 diabetes mellitus are still rising. [2]
Blacks worldwide are more likely to develop T2DM compared to Caucasians. For example, this racial disparity has been so in the United States over the past several years due to a combination of genetic, environmental, and socioeconomic factors.
Because family members share both genetics and lifestyle habits, having an immediate family member with type 2 diabetes (T2DM) increases the risk of developing the disease in children.
Babies who weigh less than 2500 g at birth are more likely to develop T2DM later in life.
African female children are more likely to develop type 2 diabetes (T2DM) than males.
The risk of childhood type 2 diabetes (T2DM) increases when a mother has diabetes during pregnancy.
The diagnosis of T2DM in children is as follows:
1. History taking
This involves your child’s doctor asking about the complaints that your child has, followed by a medical and family history of the child. The doctor may ask if the mother had diabetes while pregnant with the child or if any close family member has diabetes.
2. Physical examination
Here, a head-to-toe examination of the child is carried out. You may be asked to hold the child while the doctor checks for darkened areas around the neck and armpit. The child may also be asked to stand on a weighing scale to check for weight loss.
3. Laboratory tests
These tests can be carried out in the doctor’s office or in the laboratory. They include random or fasting blood glucose tests, oral glucose tolerance test (OGTT) and haemoglobin A1C tests. [2] Additional tests may be necessary if complications are suspected by your child’s healthcare provider.
There are several complications of T2DM in African children. They can be grouped as Acute and Chronic. Majority of the chronic complications are due to long term problems with blood vessels.
These are commonly metabolic in nature and include:
DKA and HHS may progress faster and are more fatal in children with type 2 diabetes than in adults with the disease. [2]
These include:
There are three recommended ways to prevent and manage type 2 diabetes in children according to the American Academy of Paediatrics (AAP). They include:
Modifying the lifestyle of the child involves addressing their eating habits and daily activities.
A child with type 2 diabetes should eat the same amount of food at the same time every day to prevent random spikes in blood sugar levels. Your child's doctor may refer you to a registered dietitian for guidance on the appropriate foods your child should eat. [2]
The best food for a child with type 2 diabetes should include:
The American Academy of Pediatricians (AAP) recommends an active lifestyle that includes limiting screen time to less than 2 hours per day and engaging in at least 60 minutes of moderate to vigorous exercise daily. [2]
Limiting screen time helps prevent a sedentary lifestyle and encourages physical activity. While exercise, in the right proportion improves insulin sensitivity, lowers blood glucose levels, and promotes overall health in children with type 2 diabetes.

African children playing outdoor with hand joined. Image credit: Freepik
These exercises should be fun and natural to ensure the child’s full compliance. To prevent boredom or exhaustion, you may consider splitting the recommended 60 minutes of exercise into shorter active sessions of 15–20 minutes throughout the day.
These sessions may include activities like:
However, be mindful of the risk of hypoglycemia (low blood sugar), which may occur when a child over-exercises.

Liquid metformin.
Metformin is the standard first-line drug for managing type 2 diabetes mellitus in children. It is available as a liquid. [2]
When your child is diagnosed with T2DM, the doctor may start them on metformin and gradually increase the dose every 1–2 weeks until the maximum effective dose is reached. [2]
Insulin is introduced if the child is already showing signs of diabetic ketoacidosis (DKA). This stage will require frequent monitoring of blood glucose levels to prevent hypoglycemia.
Generally, children with T2DM require higher doses of insulin, and the doctor may adjust the dosage based on blood sugar levels and the child’s response to treatment.

Closeup of a diabetic perfoming finger prick test for blood sugar level. Image credit: Freepik.
In addition to lifestyle modification and medication use, it is important that your child with type 2 diabetes mellitus undertakes regular blood sugar testing. This involves:
Daily testing provides opportunity for diabetic children and their caregivers to know if a child’s blood sugar level is within proper control at any point in time during the day and if not, to intervene promptly to bring it under control.
People in sub-Saharan Africa (SSA) face various challenges in the prevention and treatment of diabetes in children. These include:
1. Lack of awareness
Fewer people in the region know about childhood type 2 diabetes. This limited health literacy and misconceptions persist across sub-Saharan Africa and affects prevention efforts, as many communities remain unaware of modifiable risk factors and early warning signs of T2DM in children. [4]
Treatment and management of T2DM in low and middle income countries aren't subsidised like those of communicable and infectious diseases. The cost burden of the disease, which is paid out-of-pocket by families of affected children, extends beyond basic medication to include monitoring supplies and regular medical consultations, often making comprehensive diabetes management inaccessible for many families in SSA.
A major issue of public health concern is the worsening of the obesity pandemic in African children. Obesity reflects misinformed cultural embrace of well-being in many African communities. This presents a significant challenge to prevention efforts and weight management interventions for children at risk of T2DM.
African countries need to develop effective public health policies to control the rising obesity in children in the region.
Many patients in SSA lack access to the medicines, technologies, and good-quality care they need. This challenge makes early diagnosis and treatment in children with T2DM difficult. [4]
Type 2 diabetes mellitus is a metabolic disorder that develops rapidly in children when there is an imbalance between diet and physical activity. Without early intervention, the condition progresses quickly, leading to several complications with multiple organ damage. Addressing this growing problem requires increased awareness, better access to healthcare, and proactive lifestyle changes. By promoting early diagnosis, encouraging physical activity, and improving treatment accessibility, the impact of type 2 diabetes mellitus in African children can be reduced.
1. World Health Organization. Diabetes [Internet]. Geneva: WHO; Nov. 14, 2024. [Cited 2025 Feb 15]. Available from here.
2. Tillotson CV, Bowden SA, Shah M, Boktor SW. Pediatric type 2 diabetes [Internet]. StatPearls. 2023 Nov 12 [Cited 2025 Feb 15]. Available from here.
3. Diabetes UK. Physical activity and your child [Internet, n.d.]. [Cited 2025 Feb 15]. Available from here.
4. Nbarna JCN, Assah FK, Saji J, Atanga EN. Obesity and Type 2 Diabetes in Sub-Saharan Africa. Curr Diab Rep. 2014;14(7):501. doi:10.1007/s11892-014-0501-5. Available from here.
Related:
Published: March 1, 2025
© 2025. Datelinehealth Africa Inc. All rights reserved.
Permission is given to copy, use and share content for non-commercial purposes without alteration or modification and subject to source attribution.
DATELINEHEALTH AFRICA INC., is a digital publisher for informational and educational purposes and does not offer personal medical care and advice. If you have a medical problem needing routine or emergency attention, call your doctor or local emergency services immediately, or visit the nearest emergency room or the nearest hospital. You should consult your professional healthcare provider before starting any nutrition, diet, exercise, fitness, medical or wellness program mentioned or referenced in the DatelinehealthAfrica website. Click here for more disclaimer notice.


